Portosystemic Shunt Case Study
Clinical Connections – Autumn 2020
Billy, a four-month-old Jack Russell terrier, presented to his referring vets with a history of intermittent vomiting and diarrhoea, occasional hindlimb ataxia, and head bobbing. An abnormal bile acid stimulation test raised the suspicion of a portosystemic shunt.
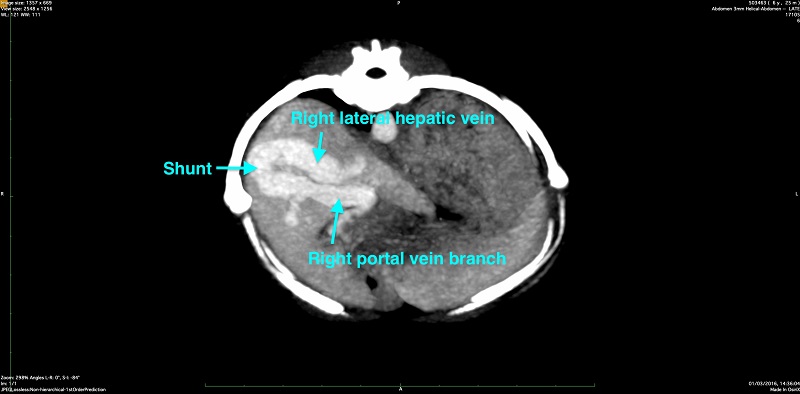
Following referral to the RVC, Billy underwent a computed tomography (CT) angiography study. This study demonstrated a single intrahepatic portosystemic shunt, originating at the right portal branch and inserting with the right lateral hepatic vein.
Following a period of medical management, Billy was readmitted to the Queen Mother Hospital for Animals (QMHA) for surgical treatment. A laparotomy was performed, and the shunting vessel was identified in the right lateral lobe of the liver.
Partial attenuation of the shunt vessel was performed using ligatures, diverting more blood from the intestines along the normal pathway to the liver rather than directly into the systemic circulation as the intrahepatic portosystemic shunt had allowed for, causing Billy’s clinical signs. A full attenuation of the shunt was not possible due to build-up of excessive blood pressure from the intestines, which is seen in about 50% of patients undergoing surgical portosystemic shunt ligation.
Billy recovered well from his surgical procedure and was released to his owner’s care with advice for rest for the next four weeks and on a strict hypoallergenic diet. Billy visited the QMHA again a month later for his follow up visit. His owners were happy to report that he had been well and the prior noted clinical signs had disappeared. An ultrasound exam of the abdomen was performed to assess residual blood flow through the partially attenuated shunt, which was found to be fully closed at that time.
Billy’s laboratory work confirmed almost complete return to normal of his previously elevated biliary values. This confirmed that his liver function had adapted well to the now established normal blood flow and was able to remove the toxins from the blood which had caused his clinical signs, as the blood was previously largely bypassing the liver through the portosystemic shunt.
Veterinary progress
Diagnosing intrahepatic portosystemic shunts is a challenge due to the complex anatomy of the hepatic and portal vasculature in the cranial abdomen. This can especially be difficult using ultrasonography, where overlying gas in the lung or stomach reflecting the ultrasound beam may provide very limited visibility of the regional anatomy. CT angiography provides cross-sectional images of the body, where specifically the vascular structures are highlighted with contrast medium – in this case the portal and systemic veins.
Using an advanced CT system, such as the QMHA’s 320 slice Canon Aquilion ONETM / GENESIS Edition CT, allows for very rapid acquisition of images. This is essential in patients that may not be able to hold their breath for long, such as patients with portosystemic shunts. Very thin image slices can be obtained, which allow for optimal review of the anatomy in multiple planes or three-dimensional reconstructions. Recently, the QMHA’s Diagnostic Imaging team was able to release a new classification system in a study with international collaborators, which defines the intrahepatic shunts based on their insertion into pre-existing hepatic venous structures.
Mark Plested, Radiologist at the QMHA, explains: “Being able to review the relatively small vascular anatomy in these patients accurately using CT angiography is essential to establish any abnormal connections of the portal to the systemic vascular circulation, allowing optimal diagnosis. Since the majority of the literature regarding intrahepatic portosystemic shunt morphology was based on the ultrasonographic assessment, lacking the three-dimensional understanding we have developed now, CT angiography has allowed us to establish a further detailed classification of the congenital intrahepatic shunts.”
Randi Drees, Associate Professor in Veterinary Diagnostic Imaging, added: “The newly established classification system for intrahepatic portosystemic shunts provides a very accessible identification pattern of these congenital abnormalities. It allows us for more efficient and consistent diagnosis and labelling of these congenital abnormalities. This leads to more effective communication of the specific finding to the surgeons, who can then be more confident and efficient in their surgical approach, allowing for shorter procedure times in these often-difficult anaesthetic patients.”