‘Dialysis’: Renal replacement therapy - Information for vets
Fact File
What is ‘dialysis’?
‘Dialysis’ is a form of extracorporeal therapy that can be used to support patients with reduced renal function. At the RVC we have a form of ‘dialysis’ called continuous (CRRT) or prolonged intermittent (PIRRT) renal replacement therapy. We are able to treat both dogs and cats (minimum 4kg) but only with acute kidney injury. We do not offer ‘dialysis’ for dogs and cats with chronic kidney disease and renal transplantation is not possible in the UK.
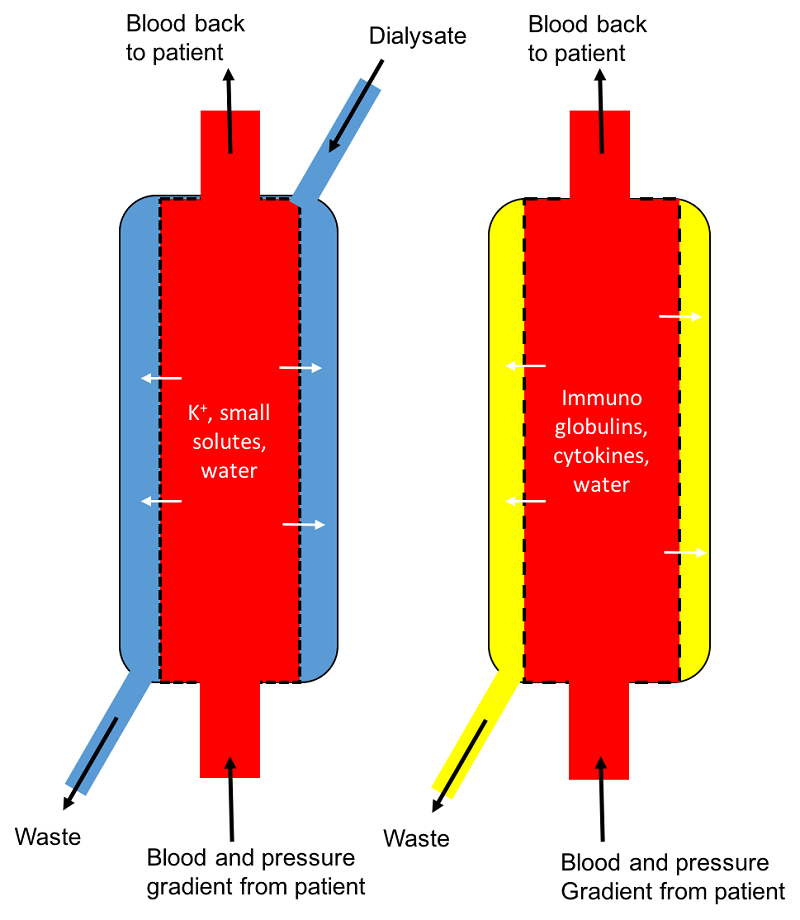
During CRRT/PIRRT blood is drawn from a large dialysis catheter placed in the jugular vein and passes round an extracorporeal circuit and through a specialised filter (Figure 1). The filter has a semi permeable membranes allowing a combination of both haemodialysis and haemofiltration to remove toxins from the blood that would normally be removed by the kidney (Figure 2). It is a more effective modality of dialysis than peritoneal dialysis for all but the smallest patients.
In very small patients, i.e. dogs or cats <4 kg we would be pleased to discuss the potential option of peritoneal dialysis.

In true CRRT, dogs or cats are connected to the machine for 18-22 hours at a time. However, it is more usual for us to perform shorter faster treatments (PIRRT) which typically take 6-8 hours to complete. When a dog or cat is receiving ‘dialysis’ they will remain in our intensive care unit being carefully monitored and will typically receive a ‘dialysis’ treatment every other day. During this time we monitor closely for evidence of improvement in renal function.
What are the main indications for CRRT/PIRRT?
The main indications for CRRT/PIRRT are acute kidney injury and toxin exposure in either dogs or cats.
Specific criteria when we consider CRRT/PIRRT in acute kidney injury patients include:
- Patients that are non-responsive to medical management of acute kidney injury
- Patients that are oligouric or anuric
- Patients with deteriorating electrolyte or acid-base abnormalities
- Patients with volume overload
Commonly, toxins that can be removed include:
- Baclofen
- NSAIDs (including Carprofen, Meloxicam, Ibuprofen)
- Selected chemotherapy agents (e.g vincristine, vinblastine)
- Ethylene glycol
For some toxins we may elect to perform plasmapheresis (therapeutic plasma exchange) rather than CRRT/PIRRT. This is dependent on the molecular size and characteristics of the toxin. We have two different machines for plasmapheresis, which allow us to perform either centrifugal or membrane plasma exchange.
Timing is critical for patients with acute kidney injury or toxin exposure and early intervention is preferable; many of these drugs may have very short half-lives, which means that we have a very narrow window for intervention. If a patient is overdosed with a drug or exposed to a toxic substance, we suggest not to wait for the toxic effects to manifest, because at that point dialysis/plasmapheresis may no longer be beneficial.
We are pleased to discuss any dog or cat where you suspect an acute kidney injury or toxin exposure, either to offer clinical advice or to discuss referral for medical therapy and/or ‘dialysis’. You can get in touch via phone on (01707) 666399 or by email us at qmhreception@rvc.ac.uk.
Is there a size restriction?
We are able to perform CRRT/PIRRT on both cats and dogs but prefer this modality of treatment for patients >4 kg. In patients <4 kg peritoneal dialysis may be considered.
What about ethylene glycol? Ethylene glycol and its metabolite glycolic acid are both readily dialyzable toxins. Patients known to have recently ingested ethylene glycol should be referred immediately for dialytic removal of these toxins which is ideally performed within 2-3 hours of exposure. If a patient has already become severely azotaemic and oligoanuric after known ingestion of ethylene glycol, damage has already occurred to the kidney CRRT/PIRRT is not recommended.
What about lily toxicity in cats and grape/raisin toxicity in dogs? At the moment it is not known whether the toxins present in lilies or raisins/grapes are dialyzable. However, such patients may benefit from CRRT/PIRRT as a supportive measure if they develop oliguric/anuric AKI. We would be pleased to discuss these cases as soon as you have concern that lily or grape/raisin ingestion may have occurred.
What about dogs with suspected CRGV/Alabama rot?
To date the prognosis for those dogs that have developed severe azoaemia with oligoanuria associated with CRGV have a grave prognosis. There are cases of less severe renal injury that have survived without requirement for ‘dialysis’ support. The decision to offer ‘dialysis’ for a suspected CRGV patient is made on an individual patient basis. Please see our CRGV fact sheet or contact us for further information.
Should I do anything in advance of sending a patient for ‘dialysis’?
Note that vascular access is very important for the ‘dialysis’ procedure. Therefore, we recommend that you preserve the jugular veins in any patient where ‘dialysis’ is an option i.e. preferentially sample from peripheral sites e.g. cephalic/saphenous vein.
How much does ‘dialysis’ cost?
The cost of referral for AKI and possible CRRT/PIRRT will depend on the underlying aetiology and the diagnostic test that are required in addition to the period of time that CRRT/PIRRT is required. We are pleased to discuss estimates for individual cases as necessary.
What is the prognosis for cats and dogs with AKI?
The prognosis for cats and dogs with AKI is dependent on the underlying aetiology. If a treatable cause can be identified e.g. leptospirosis or ureterolithiasis then prognosis can be reasonable although patients may subsequently require management for chronic kidney disease. Prognosis for patients with unknown aetiology or toxin exposure is guarded with survival rates can be <50% often despite ‘dialysis’ support.
What will happen after I refer a case for possible ‘dialysis’?
Please call to discuss any patients that you would like to refer for management of either acute kidney injury or toxin exposure. On arrival a member of the Emergency and Critical Care team will examine the patient and will liaise with the ‘dialysis’ team in the hospital. ‘Dialysis’ is a large financial and emotional investment for all involved and therefore careful discussion and counselling with the clients will take place before we agree to proceed with any form of treatment. We will keep you closely informed of the progress of the patient that you have referred.
How do I make a referral for ‘dialysis’?
Most of these cases will present as an emergency. Please contact our Emergency and Critical Care team in order to be able to arrange a referral.